
Pelvic Floor Dysfunction overview
Pelvic floor symptoms are often described in vague or conflicting ways, which makes it hard to know what is relevant and what is not. Some people are told to "just do pelvic floor exercises", while others worry that symptoms automatically mean prolapse or the need for surgery. In reality, pelvic floor dysfunction can involve muscles that are too weak, too tense, or poorly coordinated, and those patterns can feel similar without proper assessment.
Careful understanding matters because the right next step depends on what is driving the symptoms and how much they affect daily life. This guide explains what pelvic floor dysfunction means in practical terms, the common causes and risk factors (including childbirth and menopause), and how assessment typically works in the UK. It also sets out the main treatment approaches, from pelvic health physiotherapy to selected device-based or medical options, with a focus on safety, suitability, and realistic expectations.
The first step is to understand what clinicians mean by pelvic floor dysfunction and why symptoms can vary so widely.
What Is Pelvic Floor Dysfunction?
Pelvic floor dysfunction is a broad term used to describe problems with how the pelvic floor muscles work, rather than a single diagnosis. These muscles play a central role in supporting the bladder, bowel, and pelvic organs, so changes in their function can lead to a wide range of symptoms.
The role of the pelvic floor muscles
The pelvic floor is a group of muscles and connective tissues that sit at the base of the pelvis. Together, they:
-
Support the bladder, bowel, and, in women, the uterus.
-
Help control bladder and bowel emptying.
-
Contribute to sexual function and core stability.
For the pelvic floor to work properly, these muscles need to contract, relax, and coordinate at the right times. Strength alone is not enough; timing and control are equally important. This helps explain why symptoms can appear even in people who exercise regularly or feel physically strong.
What clinicians mean by dysfunction
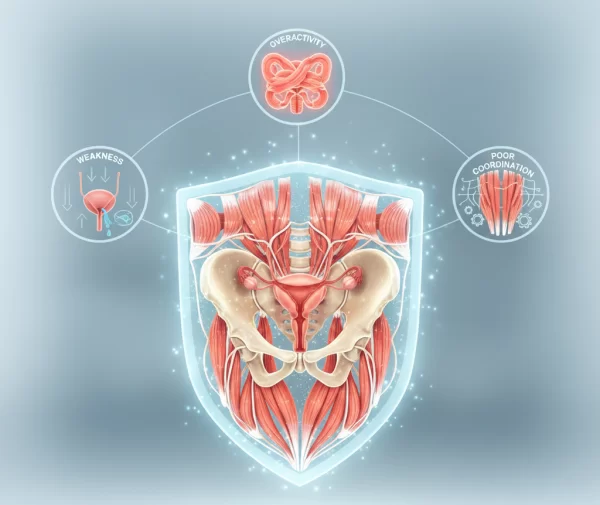
In clinical terms, pelvic floor dysfunction refers to muscles that are not functioning as they should. This may involve:
-
Weakness, where the muscles do not provide enough support or control.
-
Overactivity, where the muscles are tense and struggle to relax.
-
Poor coordination, where contraction and relaxation are mistimed.
Importantly, dysfunction does not always mean weakness. Tight or overactive muscles can cause symptoms such as pain, difficulty emptying the bladder or bowel, or even leakage. This distinction matters because treatment approaches differ depending on the underlying issue.
Pelvic floor dysfunction describes a problem with muscle function, not a single condition or outcome. Understanding how these muscles normally work helps explain why symptoms vary so widely and why assessment is an important first step.
Common Types of Pelvic Floor Dysfunction
Pelvic floor dysfunction can present in several different ways, depending on how the muscles are affected. While symptoms often overlap, clinicians generally group pelvic floor problems into a small number of patterns to guide assessment and treatment.
Pelvic floor weakness
Pelvic floor weakness occurs when the muscles are unable to provide adequate support or control. This is commonly associated with pregnancy, childbirth, menopause, pelvic surgery, or long-term strain.
Key features often include:
-
Leakage of urine during activities such as coughing, laughing, or exercise.
-
A feeling of heaviness or pressure in the pelvis.
-
Reduced control over bladder or bowel function.
Although weakness is a frequent cause of leakage, it is not the only one. This is why exercises alone are not always the right starting point without proper assessment.
Overactive or tight pelvic floor muscles
In some people, the pelvic floor muscles are overly tense and have difficulty relaxing. This pattern is sometimes overlooked because it can exist alongside symptoms that resemble weakness.
Common features may include:
-
Pelvic pain or discomfort.
-
Pain during intimacy.
-
Difficulty fully emptying the bladder or bowel.
-
Urgency or leakage is linked to poor muscle coordination rather than a lack of strength.
In these cases, strengthening exercises without guidance can worsen symptoms, making an accurate diagnosis particularly important.
Pelvic organ prolapse
Pelvic organ prolapse occurs when one or more pelvic organs move downwards due to reduced support. The degree of prolapse varies widely and does not always correlate with symptom severity.
People may notice:
-
A sensation of dragging or fullness.
-
A visible or palpable bulge.
-
Changes in bladder or bowel habits.
Many cases are mild and managed conservatively. Surgery is not always required, and treatment decisions are based on symptoms, impact on daily life, and individual preference.
Pelvic floor dysfunction is not a single condition, but a group of related patterns with different causes and management approaches. Recognising these distinctions helps avoid assumptions and supports more effective care.
Symptoms People Often Overlook or Normalise
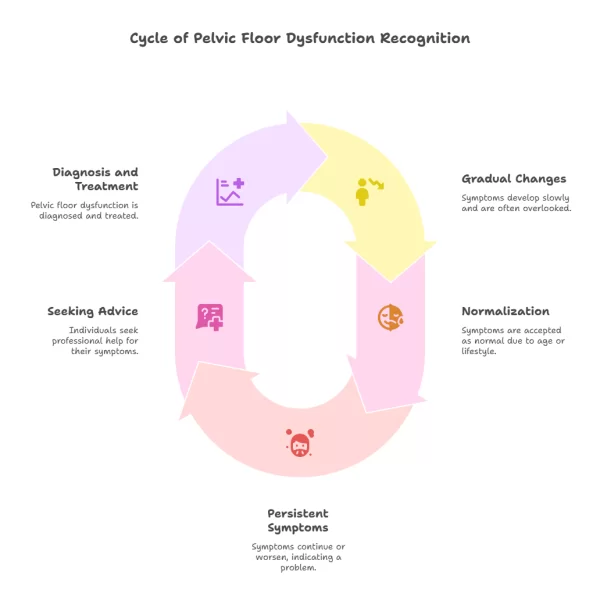
Many people live with pelvic floor symptoms for years before seeking advice, often because the changes are gradual or assumed to be an expected part of ageing, childbirth, or a busy lifestyle. Understanding which symptoms may be linked to pelvic floor dysfunction can help clarify when support is worth considering.
Bladder-related symptoms
Changes in bladder control are among the most common and most normalised signs of pelvic floor dysfunction. These may include:
-
Leaking urine when coughing, laughing, exercising, or lifting.
-
A sudden, urgent need to pass urine that is difficult to delay.
-
Passing urine more frequently than usual.
-
Feeling unable to fully empty the bladder.
Occasional leakage is often dismissed, but persistent or worsening symptoms suggest that the pelvic floor may not be working as efficiently as it should.
Bowel and core-related symptoms
Pelvic floor muscles also play a role in bowel control and core stability. When function is altered, people may notice:
-
Difficulty controlling wind.
-
Constipation or the need to strain.
-
A sensation of incomplete bowel emptying.
-
Lower back or pelvic discomfort is linked to poor core support.
Because these symptoms can feel embarrassing or unrelated, they are commonly overlooked, even when they affect daily comfort and confidence.
Pain, intimacy, and quality of life
Pelvic floor dysfunction does not always involve leakage or prolapse. In some cases, pain is the primary feature.
This may present as:
-
Ongoing pelvic pain or aching.
-
Pain during vaginal penetration.
-
Discomfort that affects intimacy or exercise.
Pain is never a symptom that should be accepted as normal. When present, it often points to muscle overactivity or coordination issues rather than weakness.
Pelvic floor symptoms are often subtle at first and easy to dismiss. Noticing patterns and persistence can help distinguish between temporary changes and issues that warrant assessment.
Causes and Risk Factors
Pelvic floor dysfunction rarely has a single cause. In most cases, it develops over time due to combined physical, hormonal, and lifestyle factors. Understanding these influences can help explain why symptoms appear and why they vary so widely between individuals.
Pregnancy, childbirth, and postnatal changes
Pregnancy and childbirth place significant strain on the pelvic floor muscles and surrounding tissues. This can include:
-
Stretching of muscles during pregnancy.
-
Muscle or nerve injury during vaginal delivery.
-
Assisted with deliveries or perineal trauma.
While many people recover well, others experience lasting changes that may not become noticeable until months or years later. Pelvic floor dysfunction can still be addressed long after childbirth, and support is not limited to the immediate postnatal period.
Hormonal changes and menopause
Hormonal shifts, particularly reduced oestrogen levels during perimenopause and menopause, can affect pelvic floor tissues. These changes may lead to:
-
Reduced tissue elasticity and strength.
-
Increased sensitivity or dryness.
-
Worsening bladder or pelvic symptoms.
Hormonal factors often interact with earlier pelvic floor strain, which helps explain why symptoms can emerge or worsen in midlife.
Lifestyle and medical factors
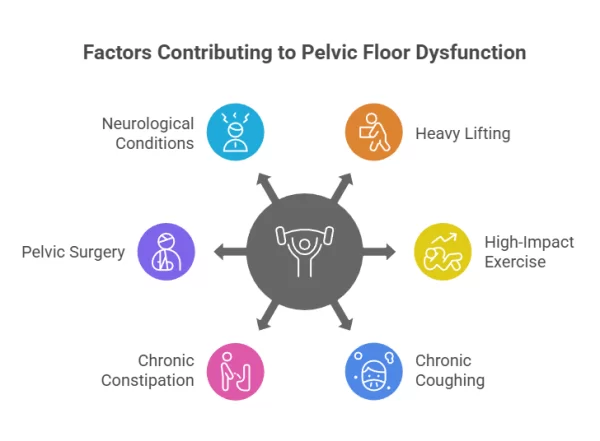
A range of everyday and medical factors can contribute to pelvic floor dysfunction, including:
-
Repeated heavy lifting or high-impact exercise.
-
Chronic coughing or constipation.
-
Previous pelvic or abdominal surgery.
-
Neurological conditions affecting muscle control.
These influences do not mean activity should be avoided, but they may require adaptation and appropriate support to reduce ongoing strain.
Pelvic floor dysfunction is usually the result of cumulative influences rather than a single event. Recognising these risk factors supports a more balanced and realistic approach to management.
How Pelvic Floor Dysfunction Is Assessed
Assessment of pelvic floor dysfunction is designed to understand how the muscles are functioning and how symptoms are affecting daily life. For most people, this process is gradual, respectful, and guided by individual comfort and consent.
Clinical assessment and referral pathways
In the UK, assessment often begins with a GP or practice nurse, who can refer to appropriate services based on symptoms. This may include referral to a pelvic health physiotherapist or, where needed, a specialist clinic.
Assessment typically involves:
-
A detailed discussion of symptoms, medical history, and lifestyle factors.
-
Questions about bladder, bowel, and pelvic health.
-
An explanation of any proposed examinations before they take place.
Physical examination is not always required at the first appointment, and patients can decline or pause assessment at any point. The focus is on understanding, not rushing to intervention.
The role of pelvic health physiotherapy
Pelvic health physiotherapists are specifically trained to assess pelvic floor muscle strength, tone, and coordination. This allows treatment to be tailored to the underlying issue rather than symptoms alone.
A physiotherapy assessment may include:
-
External and, with consent, internal examination to assess muscle function.
-
Guidance on whether muscles are weak, overactive, or poorly coordinated.
-
Discussion of personalised treatment options and expected timeframes.
This targeted approach helps avoid generic exercise advice that may be ineffective or inappropriate.
Assessment is a key step in identifying the type of pelvic floor dysfunction and guiding safe, appropriate care. For many people, this alone brings reassurance and clarity.
Treatment Options for Pelvic Floor Dysfunction
Treatment for pelvic floor dysfunction is guided by the underlying cause, symptom severity, and individual goals. In most cases, care begins with conservative approaches, with other options considered only where appropriate.
NICE guidance for the NHS recommends structured assessment and management pathways for urinary incontinence and pelvic organ prolapse, with conservative approaches often used first.
Pelvic floor exercises and physiotherapy
Pelvic floor physiotherapy is commonly the first-line approach and remains central to long-term management for many people. Treatment is tailored following assessment and may include:
-
Exercises are designed to improve strength, relaxation, or coordination, depending on muscle function.
-
Breathing and posture work to reduce unnecessary pelvic strain.
-
Education around bladder and bowel habits.
Improvement is usually gradual and may take several weeks or months. Lack of early change does not necessarily mean treatment is ineffective, but it may indicate the need for review or adjustment.
Non-surgical device-based treatments
For some individuals, non-surgical technologies may be discussed alongside or after physiotherapy. These treatments aim to stimulate pelvic floor muscles without active exercise.
Common examples include:
-
Electrical muscle stimulation is delivered via specialist chairs or devices.
-
Treatments designed to support muscle activation and neuromuscular re-education.
Such options are not suitable for everyone and should only be considered following proper assessment. Evidence quality varies, and these treatments are usually positioned as supportive rather than standalone solutions.
Medical and surgical options
In cases where symptoms are persistent or significantly affect quality of life, medical input may be required. Options can include:
-
Medications for specific bladder symptoms.
-
Pessaries for certain types of pelvic organ prolapse.
-
Surgical intervention in carefully selected cases.
These approaches are typically considered after conservative measures and involve shared decision-making based on risks, benefits, and individual circumstances.
Pelvic floor treatment is not one-size-fits-all. A stepped approach allows care to be matched to diagnosis, symptoms, and personal priorities, while avoiding unnecessary intervention.
Safety, Suitability, and Evidence Considerations
Questions about safety and effectiveness are central to any consideration of pelvic floor treatment. Understanding what is known, what varies, and what depends on individual circumstances helps support balanced, informed decisions.
Who should not pursue certain treatments
Not all pelvic floor treatments are appropriate for every individual. Suitability depends on diagnosis, medical history, and current symptoms.
Factors that may limit or delay certain treatments include:
-
Pregnancy or recent childbirth.
-
Active pelvic infection or unresolved pain.
-
Certain neurological or cardiac conditions.
-
Presence of implanted medical devices, depending on the treatment type.
This is why assessment by a qualified professional is essential before starting device-based or medical treatments.
What outcomes are realistic
Pelvic floor treatments are usually aimed at symptom improvement rather than a complete cure. Outcomes vary based on:
-
The type and severity of dysfunction.
-
Consistency with recommended therapy.
-
Lifestyle and hormonal influences.
Many people experience meaningful improvement in comfort and control, but ongoing management is common. Clear discussion of expectations helps avoid disappointment and supports long-term benefit.
Safety and suitability are as important as effectiveness. Understanding the limits of current evidence and the role of individual assessment supports more confident, realistic choices.
Pelvic Floor Health Across Life Stages
Pelvic floor health is not static. Changes in hormones, activity levels, and physical demands across adulthood can influence how the pelvic floor functions and what support is most helpful at different times.
Pelvic floor health in midlife
Midlife is a common time for pelvic floor symptoms to become more noticeable. Hormonal changes, particularly around perimenopause and menopause, can affect tissue strength and sensitivity.
People in this stage of life may experience:
-
New or worsening bladder symptoms.
-
Reduced pelvic support.
-
Increased awareness of pelvic discomfort during exercise or daily activities.
Assessment at this stage focuses on maintaining function, managing symptoms, and supporting long-term pelvic health rather than pursuing short-term fixes.
Pelvic floor health for active professionals
Younger and mid-career adults may experience pelvic floor issues linked to exercise patterns, prolonged sitting, or high physical demands at work.
Key considerations include:
-
The impact of high-impact exercise or heavy lifting.
-
Reduced movement or prolonged desk-based work.
-
Balancing fitness goals with pelvic floor protection.
Targeted advice often allows people to remain active while reducing strain, rather than stopping exercise altogether.
The pelvic floor needs to evolve over time. Regular review and appropriate support can help maintain comfort, confidence, and function across different life stages.
When to Seek Professional Support
Deciding when to seek help for pelvic floor symptoms can feel uncertain, particularly when changes have developed gradually. Clear guidance can help distinguish between symptoms that may resolve on their own and those that warrant assessment.
Signs that assessment is worthwhile
Professional input is usually helpful when symptoms are persistent, worsening, or affecting daily life. This may include:
-
Ongoing bladder or bowel leakage.
-
Pelvic pain or discomfort that does not resolve.
-
A feeling of heaviness, pressure, or bulging.
-
Symptoms that interfere with work, exercise, sleep, or intimacy.
Seeking advice does not commit you to treatment. For many people, assessment alone provides clarity and reassurance.
Choosing a qualified provider in the UK
Pelvic floor assessment and treatment should be delivered by appropriately trained and regulated professionals. This may include pelvic health physiotherapists, continence specialists, or medical practitioners with relevant expertise.
When choosing a provider, it is reasonable to ask about:
-
Professional qualifications and registration.
-
Experience with pelvic floor conditions similar to yours.
-
How assessment and treatment decisions are made.

This helps ensure care is evidence-based and aligned with your needs rather than driven by a single treatment approach. Use our specialist search to find a provider in your area.
Seeking support is about understanding options, not unnecessarily escalating care. Early, informed input often clarifies and makes management more manageable.
Supporting Pelvic Floor Health Long Term
Long-term pelvic floor health is usually supported through ongoing awareness and small, consistent adjustments rather than one-off interventions. For many people, this approach helps maintain improvements and reduce the risk of symptoms returning.
Lifestyle and self-care strategies
Everyday habits can influence pelvic floor function. Supportive strategies often include:
-
Maintaining regular, unstrained bowel habits.
-
Managing coughing or heavy lifting where possible.
-
Adapting exercise to reduce unnecessary pelvic strain while staying active.
-
Paying attention to posture and breathing patterns.
These measures are typically discussed alongside formal treatment and tailored to individual circumstances.
Building confidence and reducing stigma
Pelvic floor problems are common, yet many people avoid discussing them due to embarrassment or uncertainty. Open, factual information helps normalise these concerns and supports earlier, more effective care.
Understanding that pelvic floor management is often ongoing can reduce pressure to seek quick solutions and encourage a steadier, more confident approach to decision-making.
Supporting pelvic floor health over time is about maintaining function and comfort rather than achieving perfection. Practical, informed choices can make long-term management feel more manageable.
Conclusion
Pelvic floor dysfunction is best understood as a change in how the pelvic floor muscles work, rather than a single condition with a single solution. Symptoms can involve bladder control, bowel function, pelvic pressure, or pain, and they may reflect weakness, overactivity, or poor coordination. That distinction matters because the right support depends on what is actually driving the symptoms.
For most people, the safest starting point is a proper assessment, particularly if symptoms are persistent, affecting daily life, or causing discomfort during intimacy or exercise. Conservative care, often led by pelvic health physiotherapy, remains central for many, while other options may be considered more selectively once suitability and evidence are weighed.
If you are still unsure where your symptoms fit, it can help to note what you are experiencing and discuss it with a GP or a qualified pelvic health professional. Taking time to understand your options is a sensible step, and there is no need to rush decisions.